




Author Archives: Daniel Todd
Before and After
This patient had alar stenosis and nasal airway obstruction due primarily to a skin cancer resection. She also had a deviated septum, nasal polyps, and a boney nasal dorsal hump.


Before and After
I removed a dorsal hump and opened her sinuses at the same setting I reconstructed the nasal ala with a Melolabial flap wrapped around a conchal cartilage graft (autologous ear cartilage).


Post op Nasolabial Flap
A much improved airway after flap reconstruction. The flap includes a conchal cartilage graft to avoid collapse.


Nasolabial flap for alar reconstruction






Eosinophilic Esophagitis (EoE) Treatment Options
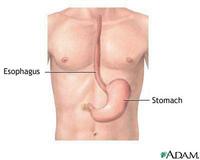 Typically allergies affect your upper respiratory tract with itchy watery eyes, sneezing, and a runny nose. This can contribute to lower airway issues such as asthma and cough. Secondly, they can lead to dermatologic manifestations such as eczema, dermatitis, and urticaria. Eosinophilic esophagitis seems to be a manifestation of allergic disease on the digestive system. It can lead to various inflammatory symptoms and even difficulty swallowing due to strictures in the esophagus.
Typically allergies affect your upper respiratory tract with itchy watery eyes, sneezing, and a runny nose. This can contribute to lower airway issues such as asthma and cough. Secondly, they can lead to dermatologic manifestations such as eczema, dermatitis, and urticaria. Eosinophilic esophagitis seems to be a manifestation of allergic disease on the digestive system. It can lead to various inflammatory symptoms and even difficulty swallowing due to strictures in the esophagus.Until recently, esophageal eosinophilia was primarily attributed to acid reflux esophagitis. Allergic patients who developed swallowing problems and intestinal symptoms underwent endosocopy and white blood cells called eosinophils were found infiltrating the mucosa. Even though we associate eosinophils with allergy, we did not make that clinical connection until recently.
In the last five years, eosinophilic esophagitis—also known as allergic esophagitis, primary eosinophilic esophagitis, and idiopathic eosinophilic esophagitis—has emerged as an important independent allergic condition found to occur in children and in adults.
Comprehensive allergy testing and immunotherapy for inhalant allergies have proven effective. That is, aggressively treating inhalant allergies with immunotherapy (allergy shots or drops) helps in treating eosinophilic esophagitis. Immunotherapy for food allergies is still being studied.
Singulair, carafate, and chromolyn may be helpful. Xolair and IL-5 inhibitor are still experimental. Food allergy testing is always completed and elimination diets are considered. A trial of an elemental amino acid diet may be entertained, but is rarely practical.
Eosinophilic Esophagitis (EoE) Treatment Options: 1) Swallowed Fluticasone. (Shake the inhaler for 15 seconds immediately before use. Do not attach a spacer. Breathe out through your mouth and then close your lips around the mouth piece. Hold your breath, press down on the top of the metal canister and swallow. Do not breath in until the medication is swallowed. After swallowing, breathe normally. Wait 15 seconds. If your were instructed to take two puffs, repeat the above steps. Replace the mouthpiece cap after each use. Do not rinse your mouth, eat or drink for 30 minutes following each use. Each inhaler contains about 120 puffs and will last 30 days taking two puffs twice daily.
You can also use Budesonide mixed with Splenda instead of Fluticasone if you like. (Open the Budesonide container and transre teh liquid into a cup. Add three to 10 packets of Splenda artificial sweetner and mix with a spoon. Swallow. Do night rinse your mouth, eat of drink for 30 minutes after taking it.) The sucralose contained in Slenda forms a thick solution that will coat the esophagus. Other artificial sweeteners do not do this.
2) Targeted dietary avoidance based on results of skin prick and patch testing to foods. If not successful, I then try empiric elimination diet. Rarely have I needed to resort to elemental diet (in a case of a child with severe oral aversion).
3) Aggressive management of aeroallergen hypersensitivity (can also trigger GI eosinophilia), that is Avoidance, Medications, and Allergy Shots. Singulair is helpful in about one half of the patients.
4) Proton Pump inhibitor (often 2 times per day) These patients generally get scoped quite frequently to monitor their progress. Dysphagia must sometimes be treated by esophageal dilatation.
Temporal Arteritis
Temporal Arteritis is also known as Giant Cell, Cranial, or Granulomatous Arteritis. It is the most common Vasculititis in the head and neck. In 50% of cases it is comorbid with Polymyalgia Rheumatica (PMR). It will often present with anemia, depression, morning stiffness and low grade fever for more than a month. It is more common in Women and more prevalent over 60. The vasculitis leads to small vessel ischemia and most notably visual loss. Patients will often have intense pulsatile cephalagia, hyperalgesia or the scalp, jaws and tongue. Masticatory claudication is very prevalent. Odynophagia, odynophonia, anorexia, fever, and streaking erythema over the temporal artery are very common. The ESR is usually over 40, and often over 100. Patients will often have high immunoglobulin counts and low albumin. A third of patients will have othamologic involvement. Early steroids are indicated and a six centimeter segment for biopsy is taken as there are skip lesions in up to 30% of patients. If the biopsy is negative and your clinical suspicion is high, might perform a biopsy on the contralateral side. If the diagnosis is made, you may have to treat with steroids up to 2 years. You never want to misdiagnose as migraines or treat with ergotomines, as the risk of blindness exists.
Endoscopic DCR
Endoscopic DCR is a relatively straightforward procedure that opens the lacrimal sac into the anterior middle meatus. I typically stent it for anywhere from 2-6 months. Afterwards, I place the patient on tobramycin drops tid for 10 days. Success should be greater than 90% and the cpt code is 31239.
Intradermal Vaccines
There has been good data on the efficacy of vaccines given intradermally vs subcutaneously or intramuscularly. It actually seems to function superiorly in children and the elderly. I personally take my flu shot this way as I feel it also limits my systemic side effects. 0.1 ml of both the influenza vaccine (Fluogen) and the Herpes Zoster Vaccine (Varivax) in opposite arms seems to lessen the frequency and severity of recurrent upper respiratory tract illnesses.
Scabies
I very experienced allergist and friend surprised me when he treated what I thought was just a heat rash with Permethrin. Scabies (Sarcoptes scabiei) is an itch mite that is highly contagious. It can be sexually transmitted for sure, but it is not always so. It does however require close contact to spread and seems limited to humans (it is not compatible with pets). Itching is severe and it forms papules that often blister. Microscopy scrapings can be difficult and there is even a PCR test available.