 Everyone has gastro-esophageal reflux (GER), the backward movement, or “reflux”, of gastric contents into the esophagus. GER can extend into the throat as regurgitation (EER), which occurs in more than 50 percent of children three months or younger at least once a day. This rate peaks at 67% at age four months.
Everyone has gastro-esophageal reflux (GER), the backward movement, or “reflux”, of gastric contents into the esophagus. GER can extend into the throat as regurgitation (EER), which occurs in more than 50 percent of children three months or younger at least once a day. This rate peaks at 67% at age four months.
Once the infant can sit up and has improved neuromuscular control, significant GER issues tend to go away. More than half of these cases resolves themselves by 10 months of age and over 80% resolve at 18 months.
However, researchers have found that 10 percent of infants with GER develop significant complications. The diseases associated with reflux are known collectively as gastro-esophageal reflux disease (GERD).
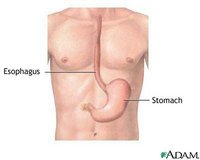
Physically, GERD occurs when a muscular valve at the lower end of the esophagus malfunctions. Normally, this muscle closes to keep acid in the stomach and out of the esophagus. The continuous entry of acid or refluxed materials into areas outside the stomach can result in significant injury to those areas. It is estimated that some 5-8% of adolescent children have GERD.
See the information about eosinophilic eophagitis on our companion site for a related topic.
What are the symptoms of GERD?
What else can cause these symptoms?
How is GERD diagnosed?
How is GERD treated?