 Keratin-filled cysts that grow medial to the tympanic membrane are considered to be congenital if they fulfill the following criteria: mass medial to the tympanic membrane,
Keratin-filled cysts that grow medial to the tympanic membrane are considered to be congenital if they fulfill the following criteria: mass medial to the tympanic membrane,
normal tympanic membrane, no previous history of ear discharge, perforation or ear surgery.
Congenital cholesteatomas occur at three important sites: the middle ear, the Petrous apex, and the cerebropontine angle. They are most often found deep to the anterior aspect of the ear drum, and a vestigial structure, the epidermoid formation, from which congenital cholesteatoma may originate, has been identified in this area.



Congenital Nasal Masses
 Congenital nasal masses are rare. Usually they represent trapped epithelial elements, primarily manifesting as epidermal inclusion cysts (63%) or dermoids. Overall, they represent 15% of dermoids. Most often they are midline as that is where congenital fusion completes itself. The higher on the nose they are the more likely the skull base involvement is. Sometimes they are deep to the nasal bones and even manifest in bifidity of the crista galli. Even some lower lesions can retain some fibrous connections to the dura. If there are significant changes to the upper or boney nose then imaging is appropriate. Often both a CT and and MRI are ordered with any anterior CNS connections. If they are low on the nose and obviously separate, I would approach them via external septorhinoplasty approach.
Congenital nasal masses are rare. Usually they represent trapped epithelial elements, primarily manifesting as epidermal inclusion cysts (63%) or dermoids. Overall, they represent 15% of dermoids. Most often they are midline as that is where congenital fusion completes itself. The higher on the nose they are the more likely the skull base involvement is. Sometimes they are deep to the nasal bones and even manifest in bifidity of the crista galli. Even some lower lesions can retain some fibrous connections to the dura. If there are significant changes to the upper or boney nose then imaging is appropriate. Often both a CT and and MRI are ordered with any anterior CNS connections. If they are low on the nose and obviously separate, I would approach them via external septorhinoplasty approach.
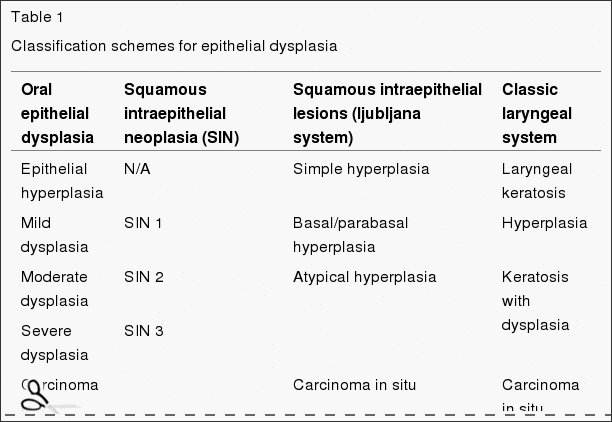
Carcinoma in Situ

Chalazion
 A chalazion (/kəˈleɪziən/; plural chalazia /kəˈleɪziə/), also known as a meibomian gland lipogranuloma, is a cyst in the eyelid that is caused by inflammation of a blocked meibomian gland, usually on the upper eyelid. Chalazia differ from styes (hordeola) in that they are subacute and usually painless nodules. They may become acutely inflamed, but unlike a stye, chalazia usually sit inside the lid rather than on the lid margin.
A chalazion (/kəˈleɪziən/; plural chalazia /kəˈleɪziə/), also known as a meibomian gland lipogranuloma, is a cyst in the eyelid that is caused by inflammation of a blocked meibomian gland, usually on the upper eyelid. Chalazia differ from styes (hordeola) in that they are subacute and usually painless nodules. They may become acutely inflamed, but unlike a stye, chalazia usually sit inside the lid rather than on the lid margin.
The Rhinoplasty Experience



Periodic Fever, Aphthous Stomatitis, Pharyngitis, Adenitis Syndrome (PFAPA)
 Periodic Fever, Apthous Stomatitis, Pharyngitis, Adenitis Syndrome (PFAPA)
Periodic Fever, Apthous Stomatitis, Pharyngitis, Adenitis Syndrome (PFAPA)
This syndrome includes recurrent episodes of fever with aphthous stomatitis (mouth sores) and pharyngitis (sore throat with redness). Occasionally, there also may be exudate (white patches on the tonsils) and usually the lymph nodes in the neck are enlarged (adenitis). Episodes of fever start suddenly and last for 3-7 days. Fevers occur routinely every few weeks; often, families know the exact day when an episode will start. Some children have other symptoms like joint pain, abdominal pain, rash, headache, vomiting or diarrhea. Children are completely well between episodes.
The disease may last for several years but usually will resolve by itself in the second decade of life. However, in nearly 15 percent of patients episodes (although less frequent) may continue to occur during adulthood. Over time, the time between the episodes will increase. Children with PFAPA continue to grow and develop normally.
It seems to be completely idiopathic, but may have some genetic component. It pretty much a clinical diagnosis. It usually ends in the second decade of life. Steroid may help and tonsillectomy and adenoidectomy is often curative.
Muscular Diastasis vs Submucous Cleft of the soft palate
 A submucous cleft palate is one type of cleft palate. The word “palate” refers to the roof of the mouth and the term “cleft” indicates a split in the palate. The palate consists of both a bony portion (hard palate) and a muscular portion (soft palate). At the end of the soft palate, the small finger-like projection of tissue that hangs down is called the “uvula”. The term “submucous” refers to the fact that the cleft is covered over by the lining (mucous membrane) of the roof of the mouth. This covering of mucosa makes the cleft difficult to see when looking in the mouth.
A submucous cleft palate is one type of cleft palate. The word “palate” refers to the roof of the mouth and the term “cleft” indicates a split in the palate. The palate consists of both a bony portion (hard palate) and a muscular portion (soft palate). At the end of the soft palate, the small finger-like projection of tissue that hangs down is called the “uvula”. The term “submucous” refers to the fact that the cleft is covered over by the lining (mucous membrane) of the roof of the mouth. This covering of mucosa makes the cleft difficult to see when looking in the mouth.
A submucous cleft of the soft palate is characterized by a midline deficiency or lack of muscular tissue and incorrect positioning of the muscles. A submucous cleft of the hard palate is defined as a bony defect in the midline or center of the bony palate. This can sometimes be felt as a notch or depression in the bony palate when the palate is palpated with a finger. Often a submucous cleft palate is associated with a bifid or cleft uvula.
Branchial Cleft Anomalies
 A branchial cleft cyst is a congenital epithelial cyst that arises on the lateral part of the neck due to failure of obliteration of the second branchial cleft (or failure of fusion of the second and third branchial arches) in embryonic development.
A branchial cleft cyst is a congenital epithelial cyst that arises on the lateral part of the neck due to failure of obliteration of the second branchial cleft (or failure of fusion of the second and third branchial arches) in embryonic development.
The cyst wall is composed of either squamous or columnar cells with lymphoid infiltrate, often with prominent germinal centers. The cyst may contain granular and keratinaceous cellular debris. Cholesterol crystals may be found in the fluid extracted from a branchial cyst. If the cyst connects to the either the skin on the outside or mucous membrane on the inside it is called a sinus. If it connects to both it is called a fistula.
Pathophysiology
Branchial cleft cysts are remnants of embryonic development and result from a failure of obliteration of one of the branchial clefts, which in fish develop into gills.
Types
First branchial cleft fistulae typically originate in the angle of the mandible and extend to the external auditory canal. They are often associated with the facial nerve. Rare ~5%.
Second branchial cleft fistulae are most common (~95%). They are found along the anterior border of the Sternocleidomastoid muscle, pass through the carotid bifurcation and into the tonsillar pillar.
Third and fourth branchial cleft fistulae are rare. The external opening occurs about 2/3 of the way down the SCM anteriorly, similar to second branchial cleft cysts. The tract ascends along the carotid sheath posteriorly to the internal carotid artery, under the glossopharyngeal nerve, and over the vagus nerve and hypoglossal nerve to open into the piriform sinus.
Symptoms
Most branchial cleft fistulae are asymptomatic, but they may become infected. The cyst, however, usually presents as a smooth, slowly enlarging lateral neck mass that may increase in size after an upper respiratory tract infection.
Treatment
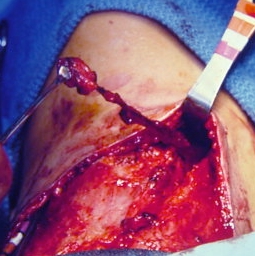 Bilateral branchial cleft sinuses during surgery. Conservative (i.e. no treatment), or surgical excision. As complete surgical excision may be difficult (due to the close proximity of the internal jugular vein and carotid vessels that lie deep to the swelling), they can recur.
Bilateral branchial cleft sinuses during surgery. Conservative (i.e. no treatment), or surgical excision. As complete surgical excision may be difficult (due to the close proximity of the internal jugular vein and carotid vessels that lie deep to the swelling), they can recur.
Frontal Sinus Surgery
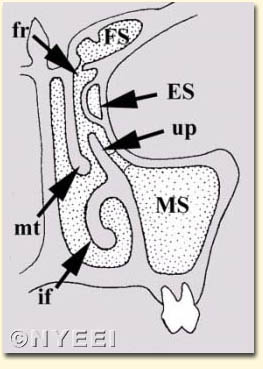
Frontal sinusotomy is a broad term which encompasses both external and intranasal approaches to open and/or create a permanent communication from the sinus to the nose.
Endoscopic frontal sinusotomy is defined as creating a permanent opening from the frontal sinus into the nose. This simple definition includes a range from relatively simple to highly complex procedures (Weber, 2001). The complexity of endoscopic frontal sinusotomy is determined by the site of obstruction to the outflow tract or disease within the sinus, and variations in frontal and ethmoid sinus anatomy.
Nose Bleed (Epistaxis)
I think most of us ENTs (in independent practice) would open our offices after hours for a colleague with a nosebleed. I’d much rather treat a nosebleed in my office than the ED (no offense meant toward my ED colleagues). I have most of the instruments and lighting that I would need there, ready to go. Definitely would favor an ED rather than a UCC.
Some “anterior” nosebleeds can bleed like stink. This is because bleeding is from a higher pressure arteriole. If you have Afrin or Neosynephrine at home (and it’s actively bleeding), I would advise using (after blowing to evacuate clots, as clot begets bleeding by depleting the clotting factors). Then firmly pinch the lower collapsible soft part of the nose (thumb and finger, tongue blades, clothes pin, I’ve even seen patients use a “chip clip”) for 10-15 minutes BY THE CLOCK. (Remember normal Ivy bleeding time is 3-10 minutes — but bleeding times are sadly no longer being done most places.)
If you have a bit of knowledge of internal nasal anatomy, you could try wetting an appropriate sized piece of cotton with decongestant and carefully slipping it into the nostril before pinching the nose. Keep the head elevated. Pressure on the upper lip below the nose can decrease the blood pressure in anterior septal arterioles. Ice on the forehead and/or back of the neck might help. If you are in the ER, use their LET Solution on a cotton ball—has the topical 1:1000 epi and is incredibly effective at constricting the offending arterioles.
Finally, and I’ve brought this up on other threads before, if you have some bacon (and no religious objections) you could cut off a generous portion (as fatty as possible) and gently stuff it snuggly into the nostril before going to the ED. Pork fat has a water soluble compound that promotes platelet adhesion (making them “super platelets”) and I have used salt pork with a number of patients on anti-coagulants as well as with thrombocytopenia. It has not failed me yet — this is after other, more “traditional” methods have failed.
Try to avoid sticking dry or abrasive materials into the nose (e.g. Kleenex, toilet paper, or even dry cotton). To prevent future bleeds I recommend: humidification, avoidance of NSAIDs (especially Toradol.
Take 250-500mg Vitamin C daily (promotes hydroxylation of proline and collagen formation).